
Most people think if a medicine makes them feel bad, it’s an allergy. But that’s not always true - and getting it wrong can put your health at risk. You might have had nausea after taking amoxicillin and told your doctor you’re allergic. Or maybe you got dizzy on a new blood pressure pill and assumed it was an immune response. The truth? You probably just experienced a side effect. Or maybe it was intolerance. And if you don’t know the difference, you could end up avoiding life-saving medications for years - or worse, end up in the hospital because you didn’t recognize a real allergic emergency.
What’s a Side Effect?
A side effect is just the body’s predictable response to how a drug works. It’s not your immune system fighting back. It’s the medicine doing its job - but also doing something you didn’t want it to do. Think of it like a car that runs well but leaks oil. The engine works fine; you just didn’t expect the mess.Common side effects include nausea, dizziness, dry mouth, drowsiness, or diarrhea. For example, about 25-30% of people who take NSAIDs like ibuprofen get stomach upset. Around 15% of those on SSRIs like sertraline feel lightheaded. And 40% of people taking older antihistamines like diphenhydramine feel sleepy. These aren’t rare. They’re documented. The American Society of Health-System Pharmacists lists over 15,000 known side effects across 1,200 medications.
The good news? Side effects often fade. Your body adjusts. You might start taking metformin with food and notice your stomach issues drop by 60%. Or you switch from a morning dose of a sedating medication to nighttime - and suddenly, you’re not dragging through the day. Side effects are usually dose-related. Take less, and they get better. Take more, and they get worse.
What’s an Allergic Reaction?
An allergic reaction is your immune system going into overdrive. It mistakes the drug for a threat - like a virus or pollen - and launches an attack. This isn’t about feeling queasy. It’s about your body going into survival mode.True drug allergies show up fast - usually within minutes to an hour. Symptoms include hives (red, itchy welts), swelling of the lips, tongue, or throat (angioedema), wheezing, trouble breathing, or a sudden drop in blood pressure. In severe cases, it’s anaphylaxis - a medical emergency that can kill within minutes if not treated with epinephrine.
Here’s the kicker: only 5-10% of people who say they have a drug allergy actually do. The CDC says 10% of Americans think they’re allergic to penicillin. But when they get tested, only 1% prove it. That’s because most people confuse nausea, rash, or headache with an allergy. A 2022 Walgreens survey found 62% of people reporting “drug allergies” were actually describing side effects - not immune reactions.
There are two types of allergic reactions: immediate and delayed. Immediate ones (Type I) are IgE-mediated and happen fast - think hives or anaphylaxis. Delayed ones (Type IV) can take days. These include rashes like DRESS (Drug Reaction with Eosinophilia and Systemic Symptoms), which can affect your liver, kidneys, and skin. DRESS has a 10% death rate if not caught early.
Once you have a true allergy, you need to avoid that drug - and sometimes others like it. Cross-reactivity matters. If you’re allergic to penicillin, you might also react to amoxicillin or cephalosporins. But not always. Testing can clear that up.
What’s Drug Intolerance?
Intolerance is the gray zone. It’s not an allergy. It’s not a classic side effect. It’s your body being unusually sensitive to a drug - even at normal doses.For example, some people get severe vomiting from codeine. Not because it’s toxic. Not because their immune system is involved. But because their liver breaks it down too fast. They’re ultra-rapid metabolizers - about 7% of Caucasians have a gene variant (CYP2D6 duplication) that turns codeine into morphine too quickly. The result? Nausea, dizziness, even breathing trouble. That’s intolerance. The same dose that helps someone else makes them sick.
Another example: aspirin-exacerbated respiratory disease (AERD). About 7% of adults with asthma develop nasal polyps and asthma attacks when they take NSAIDs like ibuprofen or aspirin. But they can usually take celecoxib - a COX-2 inhibitor - just fine. This isn’t an allergy. It’s a pharmacological mismatch. Your body can’t handle the way that drug blocks certain enzymes.
Intolerance is tricky because it’s not always clear-cut. It doesn’t show up on skin tests or blood work. Doctors diagnose it by ruling out allergy and side effects - then noticing that the reaction happens at normal doses and doesn’t get better with time. It’s not about how much you take. It’s about how your body reacts to it.
How to Tell Them Apart
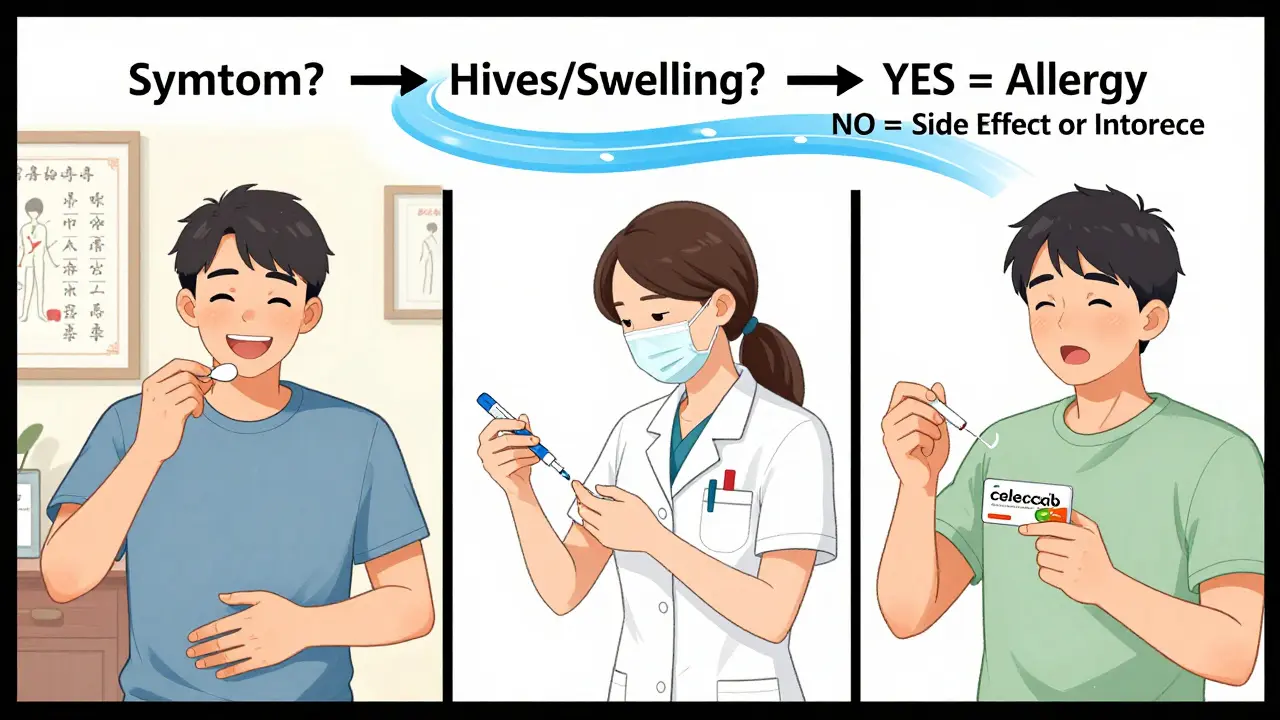
Here’s a simple way to sort them out:- Side effect? You feel sick, but it’s predictable. Nausea? Drowsiness? Headache? It happened before? It got worse when you took more? It got better when you lowered the dose or took it with food? That’s a side effect.
- Allergic reaction? You broke out in hives. Your throat swelled. You couldn’t breathe. You needed an EpiPen? You felt dizzy and passed out? That’s an allergy - even if it happened once. And you need to avoid that drug forever - until you get tested.
- Intolerance? You got sick at a normal dose, but no hives, no swelling, no breathing trouble. And you react to a whole class of drugs - like all NSAIDs - but not others? That’s likely intolerance.
Timing matters too. Allergies hit fast - within an hour. Side effects can show up anytime - even after weeks. Intolerance? Usually within hours, but not always. And unlike allergies, you can sometimes work around intolerance. Switch to a different drug in the same class. Adjust the dose. Take it differently.
Why It Matters
Getting this wrong has real consequences.If you think you’re allergic to penicillin but you’re not, you might be given stronger, more expensive antibiotics like vancomycin or clindamycin. Those drugs increase your risk of C. diff infection by 30% and MRSA by 50%. They’re also more likely to cause kidney damage or severe diarrhea. The CDC estimates that mislabeling penicillin allergies adds $2,500 per patient per year in extra costs.
And it’s not just money. A 2021 Mayo Clinic study found people with fake penicillin allergies had a 50% higher risk of surgical site infections because doctors avoided the best antibiotic. One patient in a Mayo review said she avoided all antibiotics for 15 years after one bad stomach ache - until testing proved she wasn’t allergic. She’s taken amoxicillin eight times since. No problems.
Meanwhile, if you ignore a real allergy, you could die. Anaphylaxis doesn’t wait. It doesn’t care if you’re “just a little sensitive.” It’s an emergency. And if you’ve had one, you need to carry epinephrine. Always.
What Should You Do?
If you’ve ever had a bad reaction to a drug, don’t just label it “allergy.” Get specific.- Write down what happened - hives? nausea? swelling? dizziness?
- Write down when - minutes after taking it? days later?
- Write down how bad - did you need emergency care? Epinephrine? Hospitalization?
If you had breathing trouble, swelling, or needed epinephrine - see an allergist. They can do skin tests or oral challenges to confirm or rule out a true allergy. The CDC’s three-step process (history, skin test, challenge) is safe and accurate. Penicillin testing is now routine in hospitals. The NIH even funded a new 15-minute point-of-care test coming in 2025.
If you had nausea, diarrhea, or drowsiness - talk to your doctor. Maybe you just need to take it with food. Maybe switch to a different brand. Maybe the dose is too high. You don’t need to avoid the whole class of drugs.
If you react to multiple drugs in the same family - like all NSAIDs - but no hives or breathing issues - your doctor might call it intolerance. That’s still important. But you might have alternatives. For example, if you can’t take ibuprofen, maybe acetaminophen or celecoxib is safe.
Final Thought
Medicines are powerful. But they’re not magic. They have side effects. Some people have allergies. Others have intolerances. The key isn’t to avoid everything that makes you feel weird. It’s to understand why you feel that way.Don’t let a bad stomach ache stop you from taking the right antibiotic. Don’t let fear keep you from the best treatment. And don’t assume your reaction is an allergy - unless it involved swelling, hives, or trouble breathing.
Get it right. Your body - and your future prescriptions - will thank you.
Can you outgrow a drug allergy?
Yes, especially with penicillin. Up to 80% of people who had a true penicillin allergy as children lose it over time - even if they never got tested. That’s why allergists recommend retesting every 10 years, or before major surgery. Skin tests or oral challenges can safely confirm if you’re still allergic.
Is a rash always an allergic reaction?
No. Many rashes from medications are side effects or intolerances, not allergies. A mild, flat, non-itchy rash that appears after a week or two is often a non-allergic drug reaction. True allergic rashes (like hives) are raised, red, itchy, and show up fast - within hours. If the rash is itchy, spreading, or comes with swelling or breathing issues, see a doctor immediately.
Can you be allergic to a drug you’ve taken before without problems?
Yes. Allergies can develop after repeated exposure. Your immune system doesn’t react the first time - it learns. Then, on the second or third time, it attacks. That’s why people sometimes say, “I took this before and was fine.” That doesn’t mean you’re safe now.
Should I carry an epinephrine auto-injector if I think I’m allergic to a drug?
Only if you’ve had a confirmed anaphylactic reaction - with symptoms like trouble breathing, swelling of the throat, or a sudden drop in blood pressure. If you’ve only had nausea or a rash, you don’t need one. But if you’re unsure, talk to an allergist. They’ll help you decide based on your history.
Can I get tested for drug allergies if I’m not sure?
Yes. Allergists can perform skin tests, blood tests, or oral challenges to confirm or rule out a true allergy. Penicillin testing is the most common and reliable. If you’ve been told you’re allergic but never got tested, you’re likely one of the 9 out of 10 people who aren’t actually allergic. Testing is safe, quick, and can change your medical care for life.







OMG I thought I was allergic to ibuprofen for YEARS because I got dizzy-turns out I just took it on an empty stomach. I now take it with peanut butter and life is AMAZING. Why didn’t anyone tell me this sooner???
It is imperative to distinguish between pharmacological adverse events and immunologically mediated hypersensitivity. The conflation of these entities represents a significant clinical and epidemiological error, with cascading consequences for therapeutic efficacy and public health.
My cousin in Nigeria got rash from aspirin, thought allergy. Turned out he just sensitive to the dye. Now he takes the white ones-no problem. People assume too much.
I… I didn’t know… like… hives aren’t just… like… a rash?? I thought all rashes were allergies?? I’ve been avoiding penicillin since I got a stomach ache at 12?? I’m 34 now… I think I need to go to an allergist… like… immediately??
Thank you for this clear, compassionate breakdown. Patients deserve accurate information-not fear-based assumptions. I’ve seen too many people avoid life-saving meds because they were misinformed. This post is a gift.
Side note: if you’ve been told you’re allergic to penicillin but never got tested, you’re probably one of the 90% who aren’t. Seriously-ask your doctor about a skin test. It’s quick, painless, and could save you from being stuck with antibiotics that wreck your gut. I got tested last year. Now I take amoxicillin like a champ.
Thank you for the thorough and nuanced explanation. The distinction between intolerance and allergy is profoundly underappreciated in primary care. I encourage all clinicians to prioritize patient history over self-diagnosis when documenting drug reactions.
I took Zoloft for a month and felt like a zombie. Thought I was allergic. Turns out I just needed to go slower. Started at 12.5mg and now I’m fine. Don’t panic, just adjust.
Yeah but what if the ‘side effect’ is actually your body screaming? Like… what if you’re just really good at ignoring pain until it’s too late? I think we’re oversimplifying.
My niece had a rash after amoxicillin-parents panicked, called it allergy. Turns out it was a viral rash that just happened to show up while she was on meds. She’s 8 now and takes penicillin like candy. Don’t jump to conclusions. Talk to a doctor. Not Google.
Pharmacodynamic variability, particularly in CYP450 enzyme expression, underpins many cases of apparent intolerance. The CYP2D6 ultra-rapid metabolizer phenotype, prevalent in 7% of Caucasians, results in elevated morphine concentrations following codeine administration, precipitating opioid-mediated adverse effects. This is not an IgE-mediated phenomenon.
People are so lazy. They get a little nausea and scream ‘ALLERGY!’ Then they won’t take antibiotics and get sick for weeks. If you don’t know the difference, don’t comment. Go see a real doctor. Not Reddit.
I had anaphylaxis from penicillin at 19. I had to be rushed to the ER. My throat closed. I nearly died. And now you’re telling me people are just ‘confusing side effects’? You have NO IDEA what real allergy feels like. Stop minimizing trauma.
This is the most important post I’ve read all year. If you’ve ever said ‘I’m allergic to X’ without testing, please schedule an allergist appointment. Your future self will thank you.