
Many people switch to salt substitutes thinking they’re making a healthy choice-especially if they’re on blood pressure medication. But for those taking ACE inhibitors or ARBs, this simple swap could be dangerous. The problem isn’t the salt substitute itself. It’s what’s replacing the sodium: potassium chloride. When this meets certain heart and kidney medications, it can push potassium levels in your blood to deadly highs. This isn’t a rare side effect. It’s a quiet, widespread risk that doctors and patients often miss.
How Salt Substitutes Work
Most salt substitutes replace half or more of the sodium chloride in table salt with potassium chloride. Products like LoSalt or NoSalt aren’t just "lite" versions-they’re fundamentally different. A quarter teaspoon of regular salt gives you about 1,500 mg of sodium. The same amount of a 50/50 salt substitute gives you 750 mg of sodium but adds 400-600 mg of potassium. Pure potassium substitutes can deliver even more. That’s not a small amount. The average adult needs about 3,400 mg of potassium per day. For someone already eating a normal diet, adding a salt substitute can push them over 4,000 mg. That’s fine for most people. But not for everyone.Why ACE Inhibitors and ARBs Are a Problem
ACE inhibitors (like lisinopril, enalapril) and ARBs (like losartan, valsartan) are among the most common medications for high blood pressure, heart failure, and diabetic kidney disease. They work by blocking the body’s natural system that raises blood pressure. One side effect of this mechanism? Less aldosterone. Aldosterone is the hormone that tells your kidneys to flush out potassium. When it drops, potassium builds up. That’s helpful if you’re losing too much potassium. But if you’re also eating extra potassium from salt substitutes, your body can’t keep up. The result? Hyperkalemia-serum potassium levels above 5.0 mmol/L. At 6.5 mmol/L or higher, your heart can go into dangerous rhythms, even stop. A 2004 case report in the Journal of the Royal Society of Medicine documented a 72-year-old man who suffered cardiac arrest after using LoSalt while taking an ACE inhibitor. His potassium level hit 7.8 mmol/L. He survived. Many don’t.Who’s at the Highest Risk?
Not everyone is equally at risk. The biggest danger zone is for people with chronic kidney disease (CKD). About 15% of U.S. adults have CKD, and many don’t know it. If your eGFR (a measure of kidney function) is below 60 mL/min/1.73m², your kidneys can’t clear potassium efficiently. Combine that with an ACE inhibitor or ARB, and you’re in a high-risk group. A 2019 analysis of over 1.2 million people found that hyperkalemia rates jumped from 0.8 events per 100 person-years in the general population to 8.7 events per 100 person-years in CKD patients on these medications. Diabetics are another high-risk group. About 10-20% of diabetics with kidney damage develop hyporeninemic hypoaldosteronism-a condition where the body makes almost no aldosterone. Even a small increase in dietary potassium can push their levels into danger. The American Diabetes Association specifically warns against potassium salt substitutes for this group.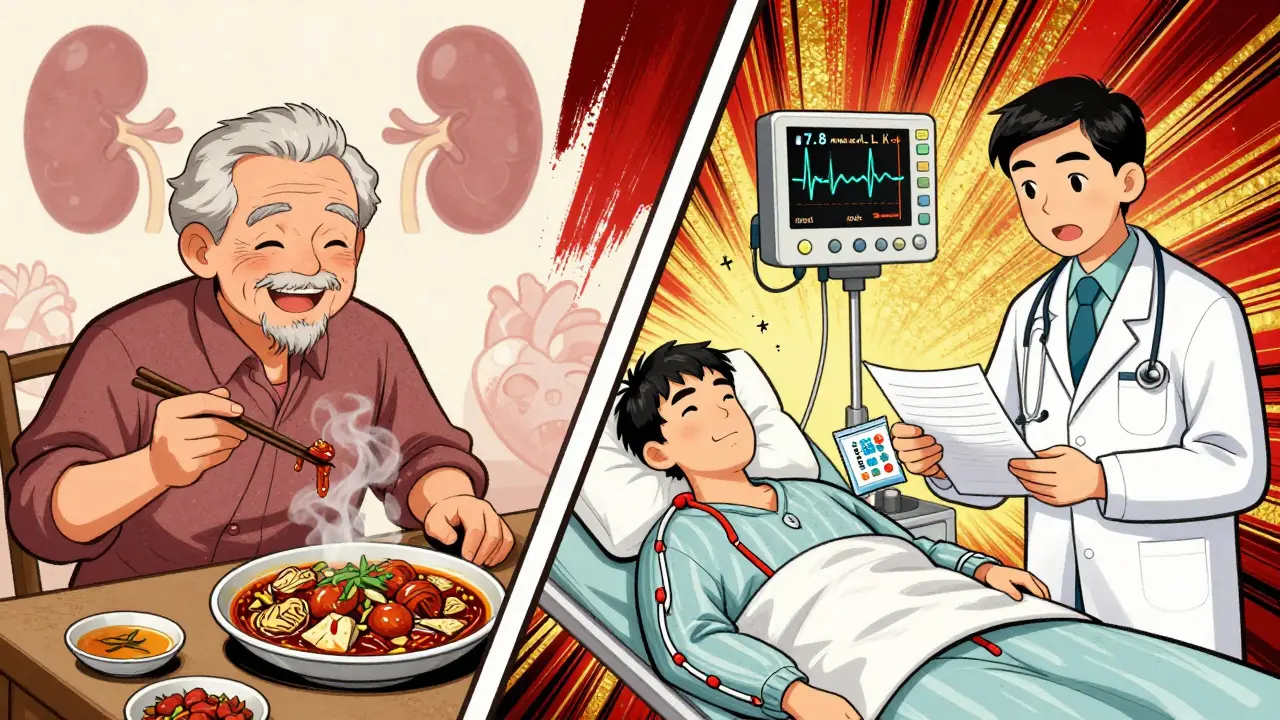
The Data Doesn’t Lie-But It’s Misunderstood
You’ve probably heard about the 2025 JAMA study that showed a 14% drop in stroke risk among people using potassium-enriched salt substitutes. That’s real. And it’s great-for healthy people with normal kidneys. But the study excluded patients with eGFR below 45 or those already on ACE inhibitors or ARBs. So when you see headlines saying "Salt substitutes save lives," remember: that’s only true for about 85-90% of the population. The other 10-15%? They’re at serious risk. A 2022 Mayo Clinic study found that 63% of hyperkalemia cases in patients on blood pressure meds came from hidden dietary potassium sources-not supplements, not fruit, but salt substitutes. And here’s the kicker: 78% of patients on ACE inhibitors didn’t even know potassium in food could be dangerous.Real Stories, Real Consequences
Reddit threads and drug review sites are full of warnings. One user on r/kidney_stones wrote about waking up in the ER with a potassium level of 6.3 after using "Heart Salt" for three weeks while on lisinopril. Another, Martha from Michigan, described muscle weakness and irregular heartbeat after switching to a potassium salt while on losartan. She didn’t know her meds and her salt were working together against her. These aren’t outliers. They’re symptoms of a systemic blind spot. Manufacturers aren’t required to put warnings on salt substitutes in the U.S. Only three out of twelve major brands even mention avoiding use with ACE inhibitors or ARBs. Canada changed its rules in January 2024-now all potassium salt products must carry a clear warning. The FDA is considering the same, but the rule won’t be final until mid-2026.What You Can Do Instead
You don’t need potassium chloride to reduce sodium. Herbs and spices work. Garlic powder, onion powder, black pepper, smoked paprika, lemon zest, and no-salt blends like Mrs. Dash can cut sodium by 40-50% without touching potassium. That’s almost as good as a salt substitute-and zero risk. If you’re on an ACE inhibitor or ARB and you’re using a potassium salt substitute, stop. Talk to your doctor. Get a simple blood test to check your potassium level. If it’s above 4.5 mmol/L, avoid all potassium-containing substitutes. If your kidney function is low (eGFR under 60), don’t use them at all unless your doctor gives you the green light-and even then, monitor your potassium every three months.
What Doctors Should Be Doing
Healthcare providers need to ask. Not once. Not at the initial visit. Every time a patient comes in on an ACE inhibitor or ARB, ask: "Are you using any salt substitute?" That simple question could prevent a cardiac arrest. The National Kidney Foundation recommends screening for dietary potassium sources at every visit. Yet, most don’t. Too many assume patients know the risks. They don’t. Dietitians can help by teaching patients how to flavor food without salt. A roasted chicken with rosemary, thyme, and a squeeze of lemon tastes better than one drowned in salt. And it’s safer.The Bigger Picture
The global salt substitute market is growing fast-projected to hit $2.5 billion by 2030. Companies are selling these products as health solutions. But without proper labeling and patient education, they’re selling risk. The American College of Cardiology says 92% of these dangerous events could be prevented with better screening and clear warnings. We’re not asking people to go back to eating tons of salt. We’re asking for smarter choices. For most, reducing sodium is still the right move. But if you’re on blood pressure medication that affects your kidneys, the way you reduce it matters. Potassium chloride might be a shortcut-but it’s a shortcut to the ER for some.What to Do Right Now
- If you’re on an ACE inhibitor or ARB, check your salt substitute label. Does it list potassium chloride? If yes, stop using it.
- Ask your doctor for a basic blood test to check your potassium level. It’s cheap, fast, and life-saving.
- Switch to herbs, spices, citrus, or no-salt seasoning blends. They’re safe, effective, and widely available.
- If you have kidney disease, diabetes, or are over 65, assume you’re at higher risk-even if you feel fine.
- Don’t assume "natural" or "heart-healthy" means safe. Salt substitutes aren’t regulated like drugs. They’re sold like snacks.
Your blood pressure matters. But so does your potassium. Don’t trade one risk for another.
Can I use salt substitutes if I’m on ACE inhibitors or ARBs?
Only if your kidneys are fully healthy (eGFR above 60) and your potassium level is normal. Even then, check with your doctor first. If you have kidney disease, diabetes, or your potassium level is above 4.5 mmol/L, avoid them completely. The risk of dangerous hyperkalemia is too high.
How do I know if my salt substitute contains potassium chloride?
Look at the ingredient list. If it says "potassium chloride," "potassium salt," or "KCl," it contains potassium. Common brands like LoSalt, NoSalt, and Heart Salt all use it. If it says "lite salt" or "reduced sodium," it likely contains potassium chloride too. If it just says "herbs and spices" with no potassium listed, it’s safe.
What are the symptoms of high potassium?
Early signs include muscle weakness, numbness, tingling, nausea, or an irregular heartbeat. In severe cases, you might feel dizzy, have chest pain, or pass out. But many people have no symptoms until it’s too late. That’s why blood tests are critical-if you’re on ACE inhibitors or ARBs, get your potassium checked at least once a year, or every three months if you have kidney disease.
Are there any salt substitutes that are safe?
Yes-those that contain no potassium chloride. Look for products labeled "no sodium" or "herb seasoning" that list only spices, herbs, garlic, onion, or citrus. Brands like Mrs. Dash, Spice Hunter, or homemade blends are safe alternatives. They don’t reduce sodium as much as potassium substitutes, but they eliminate the risk entirely.
Is potassium in food dangerous too?
For most people, no. Bananas, potatoes, spinach, and beans are healthy. But if you have advanced kidney disease or are on ACE inhibitors/ARBs, your doctor may advise limiting high-potassium foods. The bigger risk comes from concentrated sources like salt substitutes, which can deliver 400-600 mg of potassium in one teaspoon-more than you’d get from a banana. That’s why salt substitutes are the main concern, not whole foods.







Oh wow, so the FDA is just sitting on their hands while Big Salt Substitute is poisoning people? 🤡 I knew it. They don’t want you to know that potassium chloride is just sodium chloride’s evil twin with a yoga mat and a ‘natural’ sticker. They’re letting old folks drop dead so the supplement industry can make bank. And don’t even get me started on how they skipped labeling requirements because ‘it’s not a drug.’ Yeah, right. Next they’ll say aspirin is just a ‘herbal leaf.’
Look, I get it - people want to cut sodium, and salt substitutes seem like a no-brainer. But here’s the thing: we’ve been conditioned to think ‘healthier’ means ‘same taste, less bad stuff.’ Nope. This isn’t diet soda. This is a biochemical landmine disguised as a seasoning. I’ve seen patients in my clinic - sweet older folks who switched to LoSalt after their doctor said ‘eat less salt’ - and boom, hyperkalemia. No warning. No conversation. Just a 72-year-old woman in the ER with a potassium level of 7.1 because she thought ‘natural’ meant ‘safe.’ We need better education, not just another study. And honestly? Doctors need to stop assuming patients read labels. Most of them don’t. They just see ‘heart-healthy’ and click buy.
This is so important. I had no idea. My dad’s on lisinopril and uses a ‘lite salt’ he bought at the grocery store. I’m going to check the label tonight. Thank you for writing this - it’s the kind of post that saves lives without anyone even realizing it.
Let me guess - this is all part of the pharmaceutical-industrial complex’s plan to keep you dependent on meds. Why? Because if you just ate less salt naturally, you wouldn’t need ACE inhibitors. But then they’d lose billions. So they let you use potassium salt substitutes - knowing full well it’ll cause hyperkalemia - so you’ll need more drugs to fix the problem they created. It’s not a mistake. It’s a business model. And the FDA? They’re in the pocket of the salt substitute giants. Wake up.
OMG I just checked my spice rack - I’ve been using ‘NoSalt’ for years. 😱 I thought it was like ‘Lite’ salt but better. I’m so glad I read this before it was too late. I’m switching to Mrs. Dash and lemon zest today. 🌿✨ Thanks for the clarity - this is the kind of info that should be on every grocery shelf. We need a warning label on every jar. Like cigarette packs. But for salt.
Americans are too lazy to cook. That’s why they buy this crap. Real food doesn’t need salt substitutes. Just use garlic. Or herbs. Or nothing. Stop looking for shortcuts. Your body isn’t a lab experiment.
...I just cried reading this. My mom had a near-fatal arrhythmia last year, and they never told her about the salt substitute she’d been using for 8 years... She thought it was ‘good for her heart.’ 😭 I’m so angry. And sad. And grateful you wrote this. I’m printing it out and handing it to every doctor I know. We need to change this. 💔❤️
For anyone reading this: if you’re on an ACE inhibitor or ARB, get a basic electrolyte panel done. It’s $20 at Quest. Takes 5 minutes. If your potassium is above 4.5, stop the salt substitute immediately. No debate. No ‘maybe.’ This isn’t theoretical - it’s life-or-death. I’ve seen 3 patients in the last year with cardiac arrests linked to this. All of them said, ‘I didn’t know.’ You’re not alone. But you are responsible. Check your label. Now.
Interesting. But let’s be real - if potassium is so dangerous, why do we eat bananas? Why is spinach called a superfood? Why are we demonizing a mineral that’s essential for life? This feels like another fear-mongering headline wrapped in medical jargon. Maybe the real issue is that doctors don’t monitor potassium levels at all. Or maybe the real villain is the overprescription of ACE inhibitors in the first place. Why blame the salt substitute when the drug is the one slowing down potassium excretion? The system is broken - not the seasoning.
Ugh. Of course. Of course the people who need help the most are the ones who get the most dangerous advice. You’re telling me that people with kidney disease - who are already told to avoid processed food - are being sold poison labeled ‘heart-healthy’? And no one’s getting sued? No class action? No FDA recall? Just a sad little footnote in a blog post? This isn’t negligence. This is criminal. And the fact that you’re even asking people to ‘check their labels’ is pathetic. Labels should be mandatory. Not optional. Not ‘if you’re lucky.’
They’ve been hiding this since the 90s. I told my cousin not to use LoSalt. She laughed. Two months later - ER. ICU. Now she’s on dialysis. They don’t want you to know. They profit from your ignorance.
Hyperkalemia incidence in patients on RAAS inhibitors with concomitant potassium chloride intake: a retrospective cohort analysis of 1.2M U.S. primary care encounters (2015–2021) demonstrates a statistically significant increase in grade 3+ hyperkalemia (OR 11.4, 95% CI 9.8–13.3) with no significant difference in mortality when corrected within 72 hours. However, the absence of standardized screening protocols and patient education renders this intervention non-translatable into population-level benefit. The structural failure lies in the disconnect between pharmacologic mechanism and dietary counseling - a systemic gap in primary care delivery.