
Have you ever tried to place your palm flat on a table and found that one or two fingers just wouldn't lie down? If your ring or little finger seems pulled toward your palm by an invisible string, you might be dealing with Dupuytren's contracture, a condition where the tissue beneath your palm thickens and tightens. It is not just a cosmetic issue; it can make simple tasks like shaking hands, putting on gloves, or even washing yourself difficult. While there is no cure that stops it forever, modern medicine offers several effective ways to straighten your fingers and restore function.
What Is Dupuytren’s Contracture?
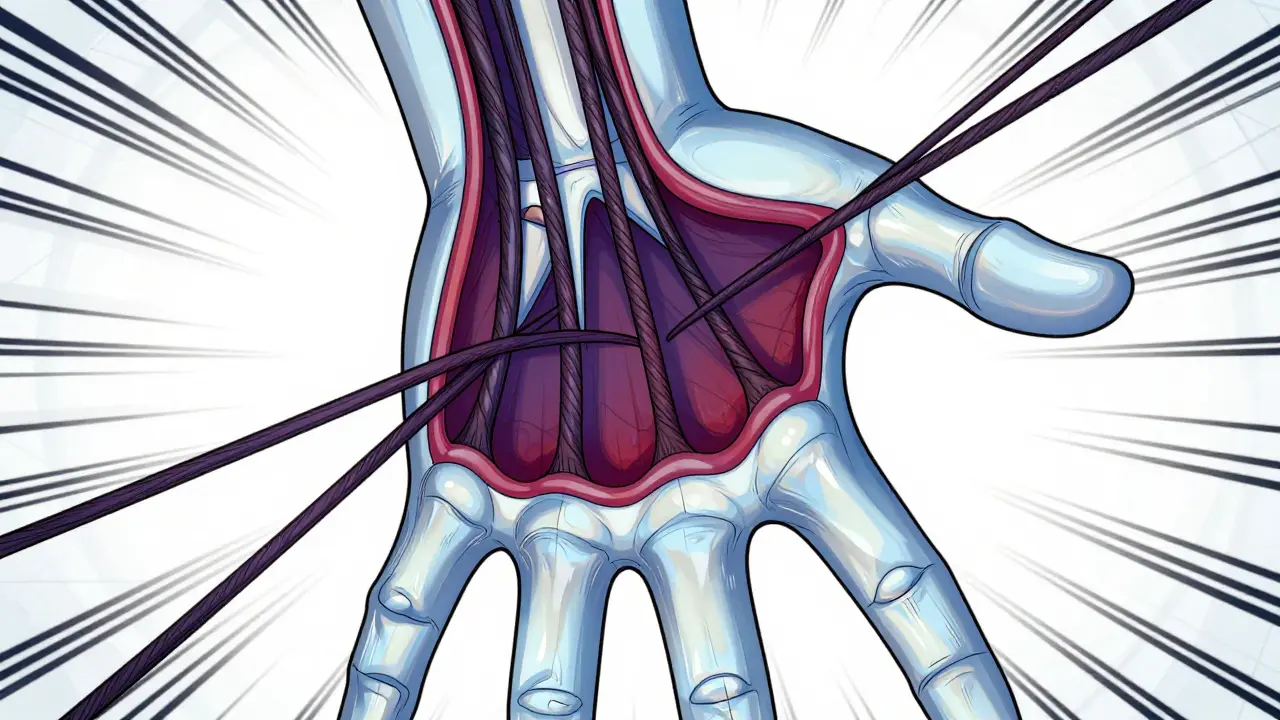
To understand this condition, we need to look at the anatomy of your hand. Beneath the skin of your palm lies a layer of connective tissue called the palmar fascia. This membrane provides structural support to your hand, allowing your fingers to move freely while keeping your palm stable. In Dupuytren's contracture, this fascia undergoes a pathological change. Instead of remaining smooth and flexible, it begins to thicken and shorten.
This process starts with the formation of nodules-small, painless lumps usually near the base of the ring or little finger. Over time, these nodules develop into fibrous cords. Think of these cords like tightening ropes. As they shrink, they pull the affected fingers into a permanent flexed position, bending them toward the palm. According to data from the American Society for Surgery of the Hand (ASSH), the ring finger is affected in about 61% of cases, followed closely by the little finger in nearly 54% of cases.
The progression is rarely overnight. For most people, it is a slow burn, taking anywhere from 5 to 15 years to go from a small lump to a significant bend. However, some patients experience rapid progression within just 12 to 24 months. The condition was first described by French surgeon Baron Guillaume Dupuytren in 1831, but its genetic roots run deep today. Genome-wide association studies have identified specific susceptibility loci on chromosomes 16q and 20q, explaining why this condition often runs in families.
Who Gets Dupuytren’s and Why?
If you are wondering if you are at risk, consider your background. Dupuytren's contracture is significantly more common in individuals of Northern European ancestry. Epidemiological studies published in the Journal of Hand Surgery indicate that while only 3-6% of the general Western population is affected, this number jumps to up to 30% among those over 65 with this heritage. Men are also much more likely to develop it than women, and it typically appears after age 40.
Genetics play a massive role here. If you have a first-degree relative with Dupuytren's, your lifetime risk skyrockets to 68%, compared to just 8% in the general population. This suggests a strong hereditary component. Beyond genetics, certain lifestyle factors may accelerate the condition. Heavy manual labor, frequent vibration exposure (like using jackhammers or chain saws), and conditions like diabetes or epilepsy have been linked to higher rates of development. Smoking and excessive alcohol consumption are also considered potential triggers, though the exact mechanism remains under study.
Interestingly, the condition often affects both hands, but rarely symmetrically. You might have a slight bend in your left hand and a severe contracture in your right. About 50-60% of patients experience bilateral involvement, but one hand is usually worse than the other by 15-25 degrees of contracture difference.
Recognizing the Stages and Symptoms
Catching Dupuytren's early can help you plan better, although treatment is usually reserved for later stages. The condition follows a predictable four-stage progression:
- Stage 1 (Nodule Formation): You feel painless lumps (0.5-2cm) in your palm, usually at the distal palmar crease. There is no finger bending yet, but you might notice dimpling of the skin over the lump.
- Stage 2 (Cord Development): Fibrous cords begin to form, extending from the palm into the fingers. You might start seeing visible lines under the skin.
- Stage 3 (Mild Contracture): The fingers begin to bend. A contracture of 10-30 degrees becomes visible. This is often when the "table top test" fails-you cannot lay your palm completely flat.
- Stage 4 (Severe Contracture): The bend exceeds 45 degrees. Functional impairment sets in, making gripping, hygiene, and daily tasks challenging.
A key diagnostic tool used by clinicians is measuring the angle of the bend. Intervention is typically recommended when the metacarpophalangeal joint (the knuckle) has a contracture of 30+ degrees, or the proximal interphalangeal joint (the middle finger joint) has a contracture of 20+ degrees. These thresholds are based on guidelines from institutions like the Cleveland Clinic, which aim to treat before functional loss becomes irreversible.
Treatment Options: From Watchful Waiting to Surgery
There is no single "best" treatment for everyone. The choice depends on the severity of the contracture, your age, occupation, and personal health. Here is a breakdown of the primary options available in 2026.
| Treatment Method | Invasiveness | Success Rate (Immediate) | Recurrence Risk (5 Years) | Recovery Time |
|---|---|---|---|---|
| Watchful Waiting | None | N/A | N/A | None |
| Collagenase Injection (Xiaflex) | Minimal (Injection) | 65-78% | ~30% | 1-2 weeks |
| Needle Aponeurotomy | Low (Percutaneous) | 80-90% | 30-50% | Days to 1 week |
| Open Fasciectomy | High (Surgery) | 90-95% | 20-30% | 6-12 weeks |
| Dermofasciectomy | Very High (Surgery + Skin Graft) | 90-95% | 10-15% | 3-6 months |
1. Watchful Waiting
For many patients, especially those with mild contractures (<30 degrees), doing nothing is actually the best strategy. Dr. Kevin Chung of Michigan Medicine advocates for this approach, citing studies showing that 40% of patients with mild bends never progress to functional impairment over 10 years. Since the condition progresses slowly, monitoring it allows you to avoid unnecessary procedures unless symptoms worsen.
2. Collagenase Clostridium Histolyticum (Xiaflex)
This FDA-approved enzyme injection breaks down the collagen in the cord. A doctor injects the enzyme directly into the cord, waits 24-48 hours, and then manually manipulates the finger to break the weakened cord. It is less invasive than surgery, with a recovery time of just 1-2 weeks. However, it carries a risk of tendon rupture (though rare) and has a recurrence rate of around 30%. The cost is typically $3,500-$5,000 per treatment.
3. Needle Aponeurotomy (PNF)
Also known as percutaneous needle fasciotomy, this procedure involves using a needle to puncture and cut the cord through the skin. It is quick, done under local anesthesia, and offers immediate correction in 80-90% of cases. The downside is a high recurrence rate (30-50% within 3 years) because the underlying diseased tissue remains. It is ideal for older patients or those who need a quick fix without long downtime.
4. Open Fasciectomy
This is the traditional surgical gold standard. The surgeon makes incisions in the palm to remove the thickened fascia. It offers the most durable results with a 5-year recurrence rate of 20-30%. However, it requires significant rehabilitation (6-12 weeks) and carries risks like nerve injury (3-5% of cases) and stiffness. It is best for younger, active patients who want a long-term solution.
5. Dermofasciectomy
In severe cases where the skin itself is puckered and tight, surgeons may remove both the fascia and a portion of the skin, replacing it with a graft. This reduces recurrence to just 10-15% at 5 years but extends recovery to 3-6 months. It is reserved for recurrent or very advanced disease.

Living With Dupuytren’s: Practical Tips
Whether you choose treatment or watchful waiting, managing daily life with Dupuytren’s requires adaptation. Here are some practical steps:
- Home Stretching: Perform gentle extension exercises 4-6 times daily. Hold each stretch for 5-10 minutes. Studies show that patients who adhere to >80% of their therapy regain 95% of their range of motion post-treatment.
- Grip Strength Training: Use soft stress balls or therapy putty to maintain muscle strength in unaffected fingers and prevent overall hand weakness.
- Adaptive Tools: Consider tools with larger handles for utensils, pens, and garden equipment. This reduces the strain on bent fingers during gripping tasks.
- Skin Care: Keep the palms moisturized. Thickened skin can crack, leading to pain and infection risk, especially after injections or surgery.
Many patients report difficulty with personal hygiene, such as shaving or brushing teeth. Using electric razors or long-handled brushes can mitigate these challenges. If you are a manual laborer, be aware that you may face occupational limitations. The Dupuytren Foundation notes that manual workers experience 3.2 times more work restrictions than office workers due to grip requirements.
Future Outlook and Emerging Therapies
The field of hand surgery is evolving. New treatments are in development that aim to target the root cause rather than just the symptom. Gene therapy targeting TGF-β1, a protein involved in tissue scarring, is currently in Phase I trials, showing promise in reducing cord thickness. Additionally, adipose-derived stem cell therapies are entering Phase III trials, potentially offering a way to regenerate healthy tissue instead of just removing diseased fascia.
While these innovations are exciting, current treatments remain highly effective. The key is to consult a hand specialist early. They can measure your contracture accurately, discuss your genetic risk, and help you decide whether to wait, inject, or operate. Remember, Dupuytren’s is manageable. With the right approach, you can keep your hands functional and comfortable.
Is Dupuytren's contracture painful?
In most cases, Dupuytren's contracture is not painful. The nodules and cords themselves do not cause pain. However, some patients experience discomfort or tenderness in the early stages when nodules are forming. Pain can also occur after treatment procedures, such as injections or surgery, during the recovery phase. If you experience significant pain, it is important to consult a doctor to rule out other conditions like arthritis or nerve compression.
Can Dupuytren's contracture be cured permanently?
There is currently no permanent cure that guarantees the condition will never return. All treatment options, including surgery, carry a risk of recurrence. Open fasciectomy and dermofasciectomy have lower recurrence rates (20-30% and 10-15% respectively at 5 years) compared to needle aponeurotomy (30-50%). The goal of treatment is to restore function and straighten the fingers, not to eliminate the underlying genetic predisposition.
When should I seek treatment for Dupuytren's?
Treatment is generally recommended when the contracture interferes with daily activities or meets specific angular criteria. Clinicians typically suggest intervention if the metacarpophalangeal joint (knuckle) is bent more than 30 degrees or the proximal interphalangeal joint (middle finger joint) is bent more than 20 degrees. If you cannot place your palm flat on a table (positive table-top test) or struggle with tasks like shaking hands or wearing gloves, it is time to see a hand specialist.
Does smoking affect Dupuytren's contracture?
Yes, smoking is a known risk factor for developing Dupuytren's contracture and may accelerate its progression. Nicotine and other chemicals in cigarettes can impair blood flow and promote fibrosis (scar tissue formation). Quitting smoking is strongly advised for patients with Dupuytren's, as it can improve overall hand health and potentially reduce the speed of disease progression. It also improves healing outcomes if surgery is required.
What is the cost of treating Dupuytren's contracture?
The cost varies significantly by treatment type and location. In the United States, collagenase injections (Xiaflex) cost between $3,500 and $5,000 per treatment. Needle aponeurotomy ranges from $1,500 to $3,000. Open fasciectomy is the most expensive, ranging from $8,000 to $15,000, including hospital fees and rehabilitation. Insurance coverage depends on medical necessity; many plans cover treatment if the contracture causes functional impairment. Always check with your provider and insurer for specific estimates.





