
When you have chronic migraine-15 or more headache days a month, with at least eight of them being full-blown migraines-your life becomes a cycle of pain, medication, and exhaustion. Pills stop working. Side effects pile up. You’re tired of guessing which day will be unbearable. That’s where Botox comes in-not as a cosmetic fix, but as a proven, FDA-approved shield against the worst of your migraines.
How Botox Stops Migraines Before They Start
Botox, or onabotulinumtoxinA, isn’t just for smoothing wrinkles. It’s a purified protein made from the botulinum toxin, the same one that causes botulism-but in tiny, controlled doses, it’s safe and effective. For migraines, it doesn’t relax muscles to make you look younger. It blocks pain signals.
Here’s how: When injected into specific spots in your head and neck, Botox enters the nerve endings and cuts off the release of key chemicals like CGRP (calcitonin gene-related peptide). CGRP is one of the main culprits behind migraine pain. It triggers inflammation, sensitizes nerves, and turns normal sensations into unbearable pain. By stopping CGRP from flooding your system, Botox prevents the chain reaction that leads to a full migraine attack.
It also interferes with SNAP-25, a protein nerves need to send pain signals. This isn’t just local-it affects the entire trigeminal nerve system, which is the main pathway for migraine pain. Studies show Botox reduces both the frequency and intensity of headaches, not just by numbing the area, but by calming the nervous system itself.
Who Gets the Most Benefit?
Not everyone with headaches qualifies. Botox is only approved for chronic migraine, not occasional tension headaches or episodic migraines (fewer than 15 headache days a month). If you’re getting migraines 15+ days a month, and over-the-counter meds or common preventives like topiramate or propranolol haven’t worked-or gave you too many side effects-Botox might be your next step.
Research shows the best responders are those who:
- Have tried and failed at least three other preventive medications
- Also suffer from medication-overuse headache (about half of chronic migraine patients do)
- Have 20 or more headache days per month (the higher the number, the more absolute relief you’ll see)
- Have comorbid conditions like chronic tension-type headache or cervical dystonia
Patients with episodic migraine (under 15 days) saw no meaningful improvement in clinical trials. That’s important. Botox isn’t a quick fix for occasional headaches. It’s a long-term strategy for those stuck in a cycle of daily pain.
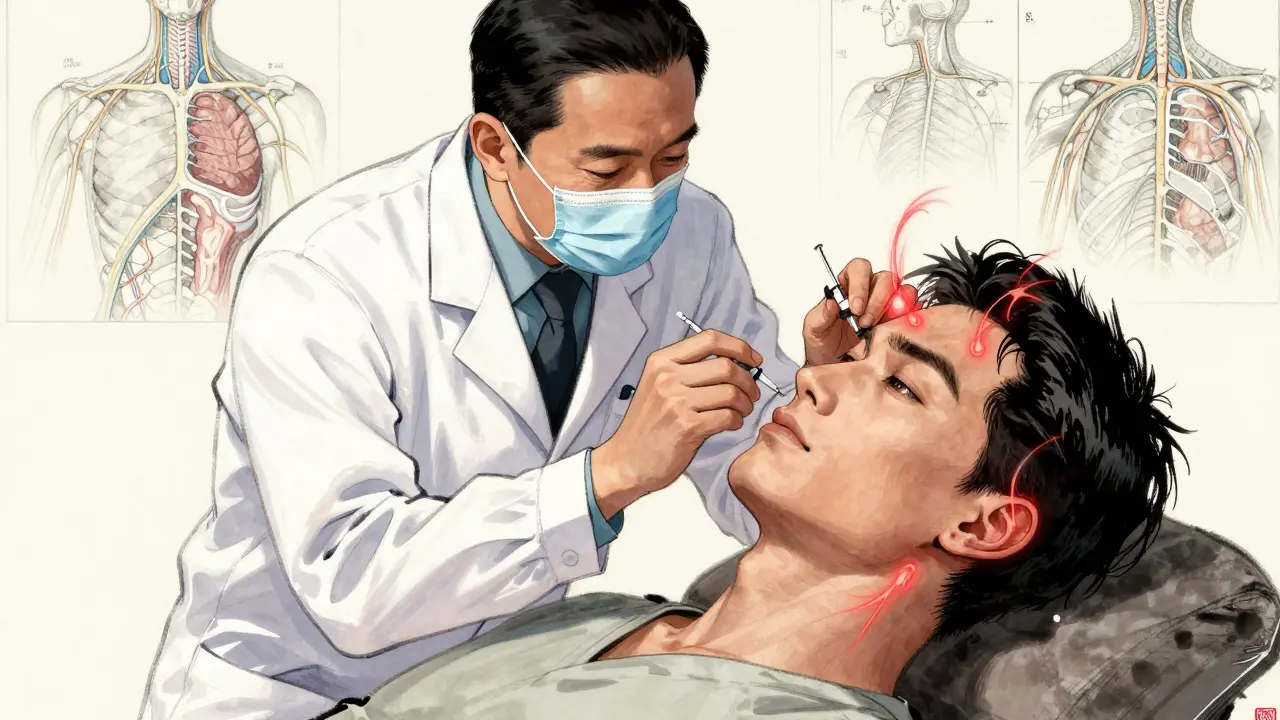
The Injection Protocol: What to Expect
The treatment isn’t complicated, but it’s precise. A trained neurologist or headache specialist gives you 31 to 39 tiny injections across seven areas: your forehead, temples, back of the head, neck, and shoulders. Each session takes about 15 minutes. No anesthesia is needed-most people describe it as a quick pinch.
The standard dose is 155 to 195 units, following the PREEMPT protocol, which is the only method proven effective in large clinical trials. Injecting in the wrong spots, or using the wrong dose, reduces effectiveness. That’s why experience matters. Studies show injector skill accounts for nearly a quarter of the outcome difference.
You get injections every 12 weeks-no more, no less. It’s not a one-and-done deal. Most people don’t feel the full effect until their third or fourth round. Patience is part of the treatment.
How Well Does It Actually Work?
Real-world results are stronger than you might think. In the original FDA trials, patients on Botox had 8 to 9 fewer headache days per month compared to 6 to 7 for those on placebo. But real-life data from over 1,200 patients shows even better results: 63% had a 50% or greater drop in headache days, with an average reduction of 12.3 days per month.
That means if you were having 25 migraine days a month, you might drop to 13. Not perfect-but life-changing. Many patients report their worst migraines now feel moderate instead of debilitating. One Reddit user wrote: “After three rounds, I went from 25 days a month to 8-10. My worst attacks are now manageable.”
The success rate? About 47% of patients achieve a 50% reduction. That’s higher than propranolol (35%) and topiramate (38%), though slightly lower than newer CGRP antibody drugs (52%). But here’s the kicker: Botox has far fewer side effects.
Side Effects and Risks: What You Might Experience
Botox is safe. Very safe. Over 12 years of use, there’s been no serious safety signal. But it’s not side-effect-free.
The most common issues:
- Neck pain (9.7%)
- Headache right after the shot (6.9%)
- Temporary eyelid droop (3.2%)
These are usually mild and go away in days or weeks. Less than 5% of people stop treatment because of side effects. Compare that to topiramate, where over a third of patients quit due to brain fog, tingling, or weight loss.
Some people report temporary muscle weakness-like difficulty raising eyebrows or holding their head up. That’s rare, and it’s a sign the injections were placed too close to certain muscles. That’s why you need a specialist, not a general dermatologist.
Cost, Insurance, and Access
Botox isn’t cheap. Each treatment costs $1,500 to $1,800. That’s $6,000 to $7,200 a year. But most major insurers cover it for chronic migraine-if you jump through the right hoops.
Insurance usually requires:
- Proof you’ve tried at least three other preventives (with documentation)
- A headache diary showing 15+ headache days per month for 3+ months
- A diagnosis from a neurologist or headache specialist
Eighty-five percent of insurers approve it when these criteria are met. But prior authorization can take weeks. Some patients wait months before getting started. That delay can be frustrating when you’re in constant pain.
There’s no generic version. Botox is the only FDA-approved botulinum toxin for migraine. Other brands like Dysport or Xeomin aren’t approved for this use-so don’t let anyone tell you they’re interchangeable.
How It Compares to Other Treatments
There are new migraine drugs-CGRP monoclonal antibodies like Aimovig, Emgality, and Ajovy. They’re injected monthly and work well. But they cost even more: $7,000 to $10,000 a year. And they’re systemic-they flood your whole body with antibodies.
Botox is local. It doesn’t affect your liver, kidneys, or hormones. That makes it ideal for people with other health conditions-like high blood pressure, depression, or kidney disease-who can’t take oral preventives.
And here’s something new: combining Botox with CGRP drugs gives even better results. A 2023 study showed 68% of patients who used both had a 50%+ reduction, compared to 51% with either alone. This combo is becoming a go-to for tough cases.
Who Should Avoid It?
Botox isn’t for everyone. Avoid it if you:
- Have episodic migraine (under 15 headache days/month)
- Are pregnant or breastfeeding (data is limited)
- Have a neuromuscular disorder like myasthenia gravis
- Are allergic to any ingredient in Botox
And don’t use it to treat an active migraine. It doesn’t work as an acute pain reliever. You still need triptans or gepants for that.
What’s Next for Botox in Migraine Care?
The FDA just approved Botox for teens aged 12 to 17 with chronic migraine-a big win for younger patients who’ve had few options. Researchers are also testing longer-lasting versions that could last 16 to 20 weeks instead of 12. That means fewer visits, less cost, and better compliance.
Scientists are now looking at “precision Botox”-tailoring injection patterns based on individual pain patterns. Maybe your pain starts in the back of your head? Maybe your neck muscles are the trigger? Future treatments might adjust the injection map to your unique biology.
For now, Botox remains one of the most reliable, well-studied options for chronic migraine. It’s not magic. It doesn’t cure anything. But for hundreds of thousands of people, it turns a life of constant pain into something manageable.
Real Stories, Real Results
On patient forums, the feedback is mixed but mostly positive. Out of 687 users surveyed, 58% said they had “significant improvement.” Many noted:
- They stopped needing daily painkillers
- They could go back to work or school
- They slept better, felt less anxious
But the complaints are real too:
- Insurance battles
- Cost
- Discomfort during injections
- Waiting months to see results
One woman wrote: “I cried after my first injection because I thought it wouldn’t work. By the third round, I was planning a vacation for the first time in five years.”
That’s the power of this treatment. It doesn’t promise a pain-free life. But it gives you back control.






People think science is magic when it works. Botox isn't curing anything. It's just silencing the noise. But silence isn't peace. It's just a pause. And we forget that pain has meaning. Maybe your body is screaming for rest. For change. For a life that doesn't revolve around headaches. We treat symptoms like enemies. But what if they're messengers?
It is with profound intellectual consternation that I observe the uncritical adoption of neurotoxins as therapeutic agents in the absence of a comprehensive understanding of the underlying pathophysiological cascades. The administration of botulinum toxin A, a substance historically associated with lethal systemic intoxication, into the trigeminal neurovascular complex represents, in my view, a paradigm of pharmaceutical reductionism that obscures the holistic nature of chronic nociceptive dysregulation.
I’ve been on Botox for 3 years now. It didn’t fix everything, but it gave me back weekends. I could play with my kids without crying. I could cook dinner without lying down for an hour after. It’s not perfect. The shots sting. Insurance fights are brutal. But if you’re drowning in pain every day, this is the life raft. You don’t have to be ‘fixed’ to be free.
They don't want you to know this but Botox for migraines is a Big Pharma trap. The real cause is EMF radiation from 5G towers messing with your cranial nerves. They use Botox because it looks scientific but it's just a band-aid to keep you coming back. They're also using it to secretly track your neural activity through the injection sites. Look up Project Nightingale. The FDA is complicit. I've got 17 years of migraine data and it all lines up with cell tower density. 😒
Been there done that. Took me 4 rounds before I felt anything. Now I go every 12 weeks like clockwork. Some days I still get headaches but they don't knock me out anymore. I don't need meds. I don't panic when the sun comes up. It's not a cure but it's a gift. Just don't go to some spa for it. Find a real headache doc. Trust me
From a neuropharmacological standpoint, the mechanism is elegantly specific: Botox cleaves SNAP-25, thereby inhibiting vesicular fusion of presynaptic neurotransmitters-including CGRP, substance P, and glutamate-within the trigeminal nucleus caudalis. This downregulates central sensitization and cortical spreading depression, which are key drivers of the migraine cascade. The PREEMPT protocol is the gold standard because it targets the nociceptive afferents in the occipital, frontal, and temporal regions with anatomical precision. Off-label injection sites yield suboptimal outcomes due to incomplete neuromodulation.
I want to say this with all the tenderness I can muster: If you're reading this and you're suffering, please don't give up. I know what it's like to stare at the ceiling at 3 a.m., counting minutes until dawn, praying for a break. Botox didn't make me 'normal'-but it made me human again. I cried the first time I remembered what it felt like to laugh without a headache. You are not broken. You are not weak. You are simply waiting for the right tool. And sometimes, that tool is a tiny needle.
It is deeply concerning how easily people accept invasive neurotoxin injections as a 'solution' without questioning the systemic failures that lead to such desperation. Why are we not investing in better access to cognitive behavioral therapy, biofeedback, or integrative neurology? Why is the medical system so quick to inject and forget? This is not healing. This is chemical pacification. And it's being sold as empowerment. I am disappointed in our collective surrender.
In my village back home, we say pain is the soul knocking on the door. But here, we knock it down with needles. Botox? It's a tool. Not a god. Not a curse. Just a way to buy time. Time to find the root. Time to rest. Time to breathe. Maybe your body isn't broken. Maybe it's just tired. And maybe, just maybe, this is the pause you need to start listening again. I respect the science. But I honor the silence between the shots.
The data is clear: Botox is only indicated for chronic migraine under strict diagnostic criteria. Any practitioner administering it for episodic headache or without documented failure of at least three preventive therapies is acting outside the standard of care. This is not anecdotal medicine. This is not wellness culture. This is neurology. If you are not meeting the ICHD-3 diagnostic thresholds, you are not a candidate. Period.
To everyone sharing their stories: thank you. Your courage is quiet but immense. This isn't just about a treatment-it's about dignity. About reclaiming hours, days, months. I’ve worked with patients who went from bedridden to teaching again. From silent to singing in the shower. Botox doesn’t erase pain. But it gives space for something else to grow. And that space? That’s where healing begins.