
A sudden spike in blood pressure that hits 200 mmHg during a routine doctor’s visit. A pounding heart with no exercise. Sweating so bad you change clothes midday. Headaches so intense they feel like your skull is splitting open. These aren’t signs of stress or anxiety-they could be symptoms of pheochromocytoma, a rare tumor hiding in your adrenal gland.
Most people with high blood pressure never find out why. Their doctors call it "essential hypertension" and prescribe pills to manage it for life. But for about 1 in every 200 hypertensive patients, the real cause is a tiny, hormone-spewing tumor called a pheochromocytoma. And here’s the kicker: once you find it, you can cure it-with surgery.
What Exactly Is a Pheochromocytoma?
Pheochromocytoma is a tumor that grows in the adrenal medulla, the inner part of the adrenal glands sitting right on top of your kidneys. These glands normally make adrenaline and noradrenaline-hormones that help you react to danger. But when a tumor forms, it doesn’t know when to stop. It floods your body with these hormones, even when you’re sitting quietly watching TV.
The result? Your body thinks it’s under attack. Your heart races. Blood vessels squeeze shut. Blood pressure rockets. You feel like you’re having a panic attack, but there’s no trigger. These episodes, called "spells," can last minutes or hours. They often happen during physical activity, emotional stress, or even while using the bathroom-if the tumor is in the bladder wall (a rare variant called a paraganglioma).
Doctors call this the "classic triad": severe headaches, drenching sweats, and rapid heartbeat. About 85% of patients get headaches. Three out of four sweat through their shirts. Most feel their heart pounding like a drum. But many don’t connect the dots. For years, patients are told they have anxiety, migraines, or panic disorder. The average delay in diagnosis? Over three years.
Why This Tumor Is So Dangerous
It’s not just the discomfort. A sudden surge of adrenaline can trigger a hypertensive crisis-blood pressure so high it can cause stroke, heart attack, or even sudden death. That’s why surgery can’t be rushed. You can’t just cut out the tumor without preparation.
Before surgery, patients need at least seven to fourteen days of alpha-blocker medication, usually phenoxybenzamine. This drug relaxes blood vessels and prevents the dangerous spikes during surgery. Skipping this step? It’s like trying to defuse a bomb without cutting the right wire. Intraoperative hypertensive crisis without proper blockade has a mortality rate of 30-50%.
But there’s more. Most people with pheochromocytoma have lost 20-30% of their blood volume because their vessels have been squeezed tight for months or years. So before surgery, doctors also push patients to drink 2-3 liters of water daily and eat a high-sodium diet. This expands the blood volume so your body doesn’t crash when the tumor is removed.
How Is It Diagnosed?
Forget blood pressure readings alone. The real diagnostic gold standard is measuring metanephrines-the breakdown products of adrenaline and noradrenaline. The two best tests are:
- 24-hour urinary fractionated metanephrines (96-99% sensitive)
- Plasma-free metanephrines (97% sensitive)
These tests are far more reliable than trying to catch a spike in blood pressure during a doctor’s visit. A reading three times above the upper limit of normal is considered diagnostic. Anything borderline? Doctors need to be cautious. About 15-20% of borderline results lead to unnecessary scans and anxiety.
Imaging comes next-after biochemical confirmation. CT or MRI scans locate the tumor. But newer tools like 68Ga-DOTATATE PET/CT are becoming standard because they’re more accurate, especially for small or extra-adrenal tumors. The "10-10-10 rule" still applies: 10% of cases are bilateral, 10% are outside the adrenal gland, and 10% are malignant. But newer data suggests up to 30% of hereditary cases are multifocal.
Is It Cancer?
Most pheochromocytomas-about 90%-are benign. But here’s the twist: you can’t always tell just by looking at the tumor under a microscope. The real red flag is whether it spreads. Metastasis to lymph nodes, liver, lungs, or bones confirms malignancy. That’s why genetic testing is now mandatory for every patient.
About 35-40% of cases are inherited. Mutations in genes like SDHB, SDHD, VHL, RET, and NF1 are common. SDHB mutations carry the highest risk-up to 50% chance of developing aggressive, metastatic disease. That’s why every patient gets genetic testing, even with no family history. Recent studies show 25% of "sporadic" cases actually have hidden mutations.
If it’s malignant, surgery still helps, but long-term survival drops sharply. Five-year survival for metastatic disease is only about 50%. New treatments like 177Lu-DOTATATE (a targeted radiation therapy) are showing promise, with response rates near 65% in early trials.
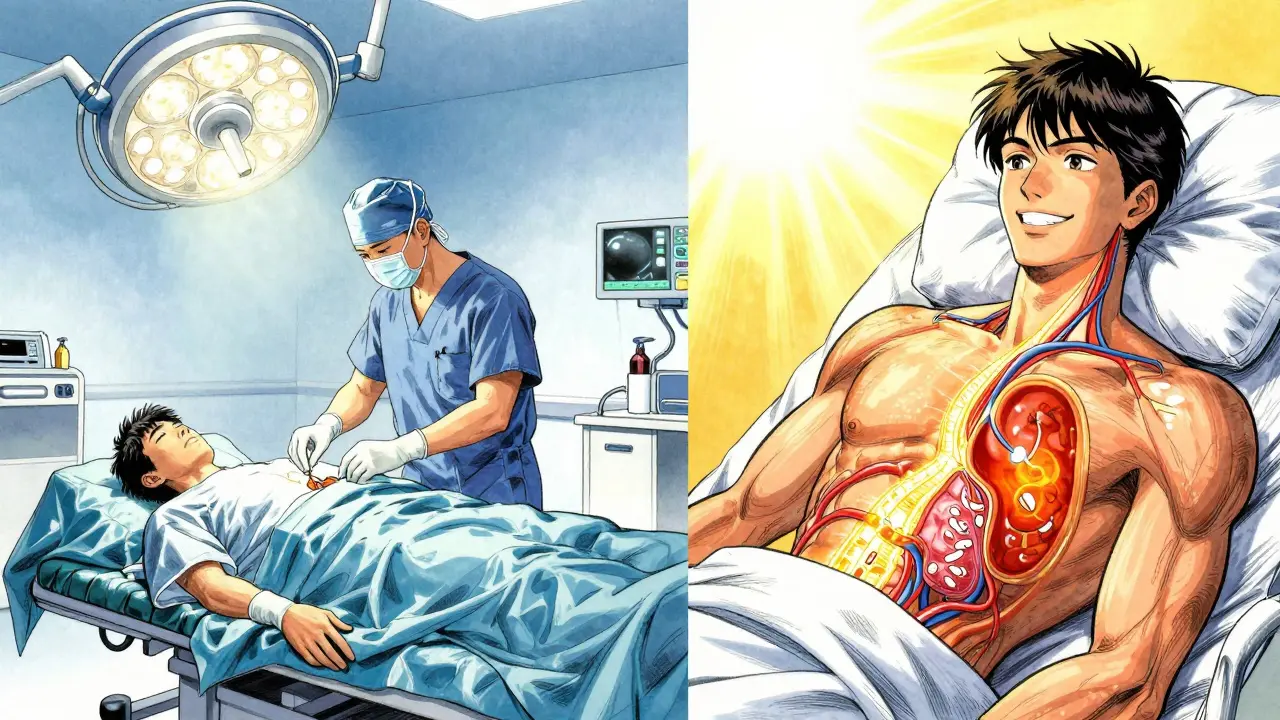
The Surgery: What to Expect
For most patients, surgery is laparoscopic-small incisions, camera, and instruments. At high-volume centers, this is done in 85% of unilateral cases. Recovery is quick: most go home in 1-2 days. Many return to work within two weeks.
But complications happen. About 5-8% of laparoscopic cases need to be switched to open surgery due to bleeding or tumor sticking to nearby organs. In rare cases, both adrenal glands are removed-especially if the tumor is bilateral or malignant. That means lifelong steroid replacement: hydrocortisone and fludrocortisone. Patients describe this as a "new normal"-constant monitoring, medication adjustments, and fatigue that lasts months.
One patient on a support forum wrote: "I was off all blood pressure meds in three weeks. My energy came back. But now I take pills every morning just to stay alive. I’d do it again in a heartbeat."
What Happens After Surgery?
For benign, single-sided tumors, the cure rate is 85-90%. Blood pressure normalizes. Medications stop. Many patients say they feel like a different person.
But follow-up is critical. Even after successful surgery, patients need annual checks for recurrence. Those with SDHB mutations need whole-body MRIs every year. The risk of new tumors doesn’t disappear.
Long-term, 12% of patients report chronic fatigue lasting over six months. Some deal with low cortisol levels, anxiety, or sleep issues. Psychological support is often overlooked but vital. Many spent years being told their symptoms were "all in their head." That trauma doesn’t vanish after surgery.
How It Compares to Other Causes of High Blood Pressure
Essential hypertension affects nearly half of American adults. It’s steady, silent, and managed with lifelong meds. Pheochromocytoma is the opposite-episodic, dramatic, and curable.
Other secondary causes like kidney artery narrowing or aldosterone-producing tumors don’t cause sweating or palpitations. Migraines and panic disorders mimic the symptoms, but they don’t show elevated metanephrines. That’s why testing is the gatekeeper. No metanephrine surge? It’s not pheochromocytoma.
Who Should Get Tested?
If you have high blood pressure that’s hard to control, especially with:
- Episodic headaches
- Unexplained sweating
- Heart palpitations without cause
- Weight loss despite normal appetite
- Family history of adrenal tumors or related cancers
Then talk to your doctor about metanephrine testing. It’s simple. It’s non-invasive. And if you have this tumor, it could save your life.
What’s Next for Treatment?
Research is moving fast. Drugs like Belzutifan, originally developed for kidney cancer in VHL patients, are now being tested for pheochromocytoma. Liquid biopsies to detect tumor DNA in blood could one day replace scans. And targeted radiation therapies are giving new hope to those with metastatic disease.
The big goal? Catch it earlier. Stop the three-year diagnostic delay. Make genetic testing routine. Train more doctors to recognize the triad. Because when you do, you’re not just treating a tumor-you’re undoing years of suffering.






I mean, sure, it's rare... but have you ever considered that maybe your body is just screaming for a vacation? 🤔 Like, what if all these 'spells' are just your soul trying to escape modern life? I once had a headache so bad I cried in a Target parking lot. Turns out I just needed to move to Bali. 🌴✨
This is actually beautiful. I work with patients who’ve been misdiagnosed for years, and this post captures the emotional weight better than any medical journal. Thank you for writing it. 💛
Surgery fixes it? Yeah right. You think they tell you the whole story? The real cost is losing your sense of self. And the meds? They're just a different kind of prison.
OMG I thought i was going crazy!! I had sweats and heart racing for 2 years... doc said anxiety... i even went to therapy... then one day i just passed out in the shower. Turns out my adrenal was doing the cha cha. Surgery saved me. now i take 2 pills a day and i dont care. alive is alive. 🙌
Thank you for this incredibly thorough and compassionate breakdown. As a healthcare provider, I’ve seen too many patients dismissed for years. This is exactly the kind of education that saves lives. Well done.
They just want you on pills forever. This is Big Pharma’s dream. You think they want you cured? No. They want you dependent. Adrenal gland? Just cut it out. Easy. Profit.
I live in Winnipeg. We get cold here. Like, 'your nose hair freezes' cold. So when I read about sweating through shirts in the middle of winter... I thought, 'this person must be from Arizona.' Then I realized - it's not the weather. It's the tumor. That's wild. And terrifying. And kind of beautiful.
It makes me wonder... if we’re all just biochemical machines, then what does it mean to be 'normal'? If a tumor makes you feel alive in the worst way possible... is that still sickness? Or just a different kind of truth?
this was so cool i learned so much lol i had no idea about the metanephrines thing
I used to feel like my body was betraying me. Every time I laughed, my heart would race. Every time I stood up, I’d sweat like I’d run a marathon. They called me dramatic. I called it survival. Now I’m on hydrocortisone and I still cry at commercials. It’s not cured. It’s just... managed. And that’s okay.
The fact that 25% of so-called sporadic cases have hidden mutations changes everything. We’ve been treating symptoms like they’re the enemy. But the real enemy is ignorance. Genetic testing should be mandatory after any unexplained hypertension. Not optional. Not 'if you're suspicious.' Mandatory.
So... you’re telling me the government doesn’t want us to know about this? Because if they did, then people would stop buying blood pressure meds? And then... what? Do they just... let us die? Or is this all just a cover-up for the alien hormone experiment in Area 51? 🤔👽
The assertion that metanephrine testing is the gold standard is empirically accurate; however, the omission of the confounding factors - such as beta-blocker interference, stress-induced elevations, and renal insufficiency - constitutes a significant oversight in clinical education. Furthermore, the assertion that surgery yields an 85–90% cure rate is misleading without specifying the inclusion criteria of the cohort. In real-world practice, comorbidity burden substantially reduces efficacy.
I'm a lab tech in Lagos. We don't have 68Ga-DOTATATE PET/CT here. We use urine metanephrines and ultrasound. It's crude. But it works. We found three cases last year. One was a 14-year-old girl. She was misdiagnosed for four years as having panic attacks. Now she's back in school. No meds. Just a scar and a second chance. This isn't just medicine. It's justice.