- CAD is primarily caused by atherosclerosis-the buildup of plaque in arterial walls.
- Risk factors include diabetes, high BMI, and smoking.
- Diagnosis often involves ECGs, stress tests, or coronary angiography.
- Treatment ranges from lifestyle changes and meds to stents (PCI) or bypass surgery (CABG).
- Risk is categorized into Low, Intermediate, and High based on the yearly chance of a heart attack.
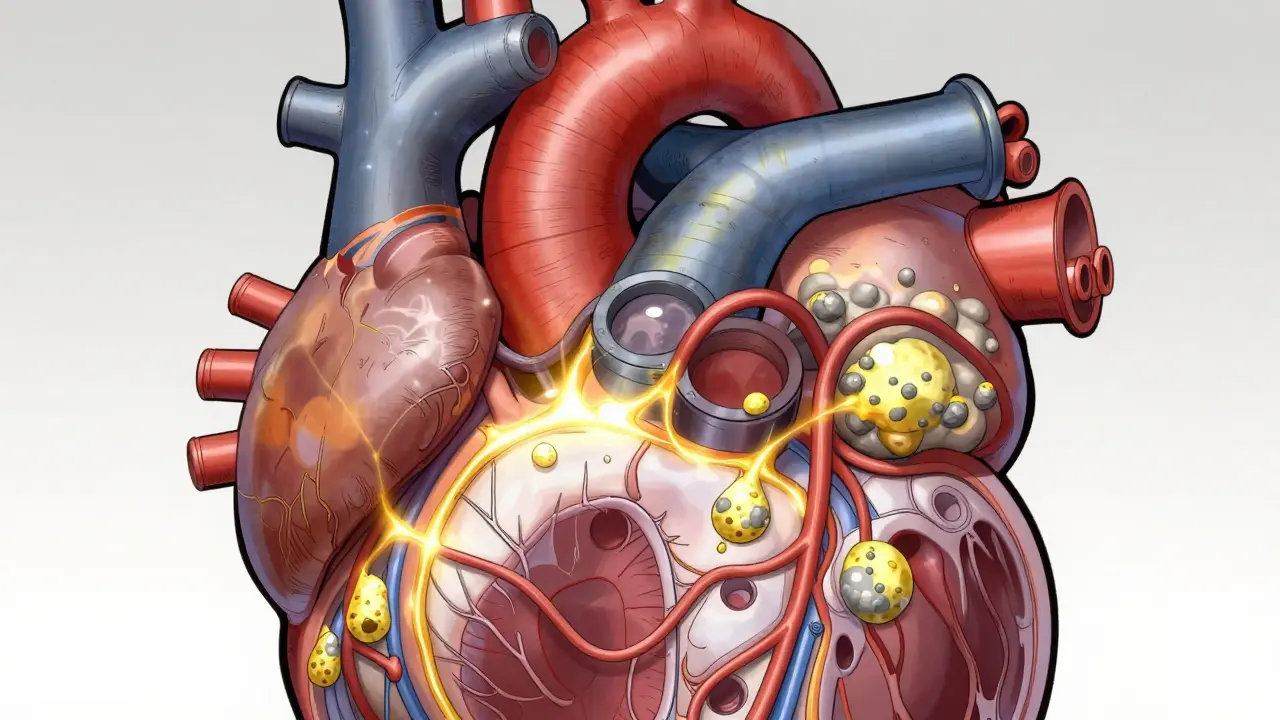
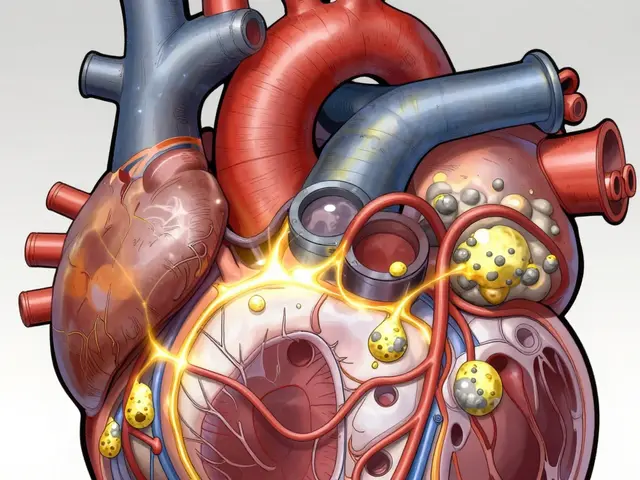
The Silent Build-Up: What is Atherosclerosis?
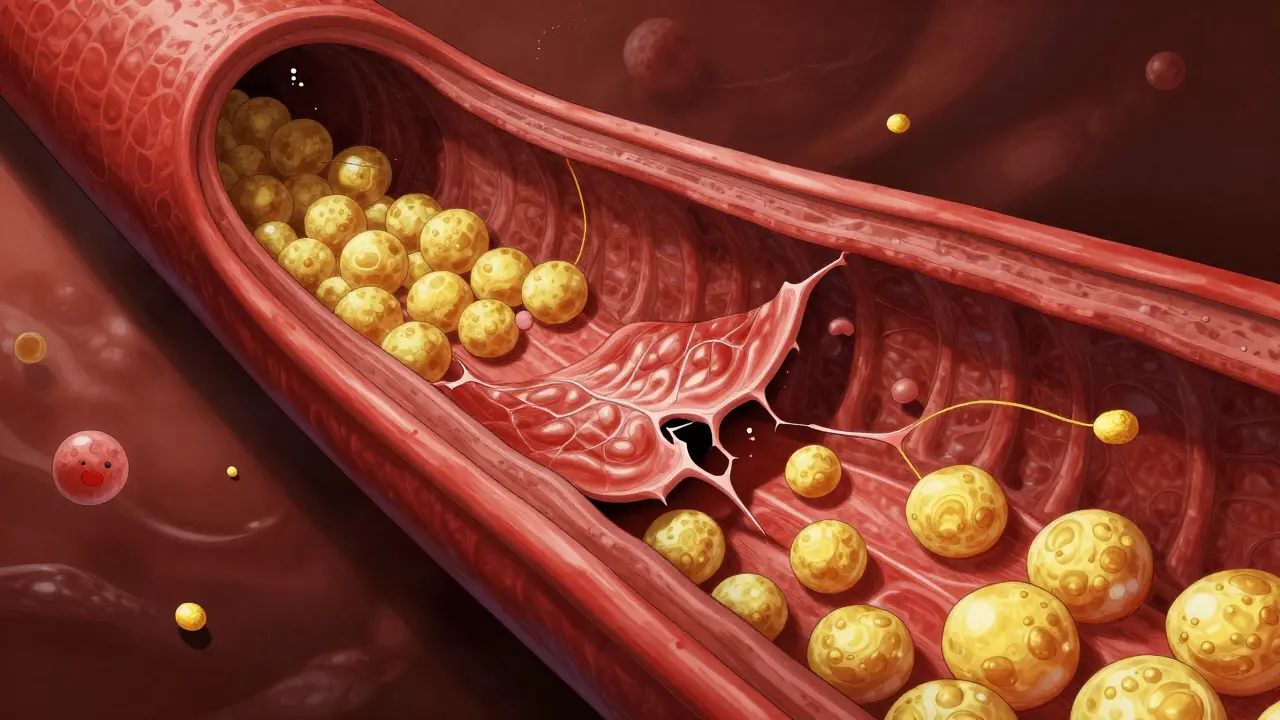
To understand CAD, you first have to understand Atherosclerosis. Think of it like old plumbing in a house where minerals build up inside the pipes. In your body, this process starts when the inner lining of your artery (the endothelium) gets damaged. Once damaged, Low-Density Lipoprotein (LDL)-often called "bad" cholesterol-seeps into the wall. Your immune system tries to help by sending inflammatory cells to clean up the LDL. However, these cells can get stuck, creating a fatty streak. Over time, this evolves into a complex plaque consisting of cholesterol, fat, and calcium. Here is the part that catches many people off guard: not all plaques are the same. You might have a "stable" plaque that narrows the artery by more than 50%, causing predictable pain when you exercise (stable angina). Or, you could have an "unstable" plaque that only narrows the vessel by 30% but has a thin, fragile cap. If that cap ruptures, it triggers a blood clot that can instantly block the artery, leading to a heart attack. This is why some people with "mild" blockages can still suffer sudden cardiac events.Who is at Risk? Knowing Your Numbers
Not everyone is equally likely to develop CAD. Doctors look at a mix of things you can control and things you can't. The 2023 ACC/AHA guidelines emphasize that risk isn't just a "yes or no" checkbox; it is a spectrum. Common risk factors include:- Metabolic Issues: Diabetes and dyslipidemia (unhealthy lipid levels) are huge drivers. Diabetes, in particular, damages the blood vessels and makes plaque buildup faster.
- Physical Markers: An elevated BMI and high blood pressure put constant stress on the arterial walls.
- Lifestyle Choices: Smoking is a primary culprit, contributing not only to CAD but also to chronic kidney disease.
- Medical History: If you have already had a myocardial infarction (heart attack) or have atrial fibrillation, your risk for further events increases significantly.
How Doctors Find the Blockage
Since you can't "feel" a plaque forming, diagnosis relies on a few key tools. If you tell a doctor you're feeling shortness of breath or chest tightness, they usually start with non-invasive tests.An Electrocardiogram (ECG) is typically the first stop. It records the electrical activity of your heart and can show if the heart muscle has been damaged or if it's struggling to get enough oxygen. If the ECG is inconclusive, a stress test might follow, where your heart is monitored while you walk on a treadmill or take medication to mimic exercise.
When a more detailed map is needed, doctors use Coronary Angiography. This is an invasive procedure where a contrast dye is injected into the arteries and viewed under X-rays. It allows surgeons to see exactly where the blockage is and how narrow the vessel has become. For those who also have leg pain or numbness, doctors might use an Ankle-Brachial Index (ABI) test to see if peripheral artery disease is also present, as these conditions often travel together.| Test | What it Measures | Invasiveness | Best For... |
|---|---|---|---|
| ECG | Electrical activity | Non-invasive | Quick screening and heart rhythm |
| Stress Test | Heart performance under load | Non-invasive | Detecting ischemia during activity |
| Angiography | Physical arterial structure | Invasive | Mapping exact blockage locations |
| ABI Test | Blood pressure in limbs | Non-invasive | Checking for Peripheral Artery Disease |
Fixing the Pipes: Treatment Strategies
Treatment for CAD isn't a one-size-fits-all deal. It's a combination of "maintenance" to stop the disease from getting worse and "interventions" to fix existing blockages.Lifestyle and Medication
The first line of defense is always lifestyle. This means switching to a heart-healthy diet (think Mediterranean style) and regular exercise. Medications are used to manage the risk factors we discussed earlier. Statins are commonly used to lower LDL cholesterol and stabilize plaques so they don't rupture. Blood pressure meds and antiplatelet therapies (like aspirin) help prevent clots from forming on existing plaques.Surgical Interventions
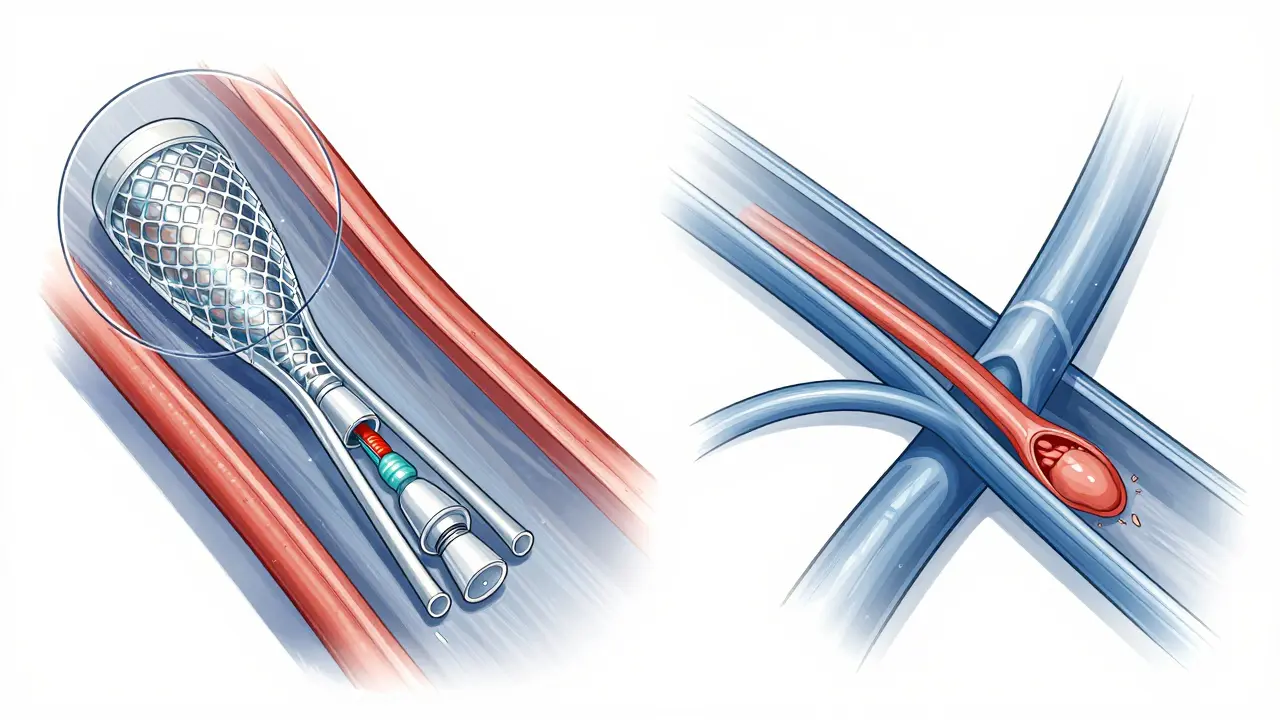
When medication isn't enough, or when a blockage is critical, doctors turn to procedures:- Percutaneous Coronary Intervention (PCI): This is a common procedure where a cardiologist inserts a catheter into an artery and uses a small balloon to push the plaque against the wall. A tiny mesh tube, called a Stent, is usually left behind to keep the artery open.
- Coronary Artery Bypass Grafting (CABG): If multiple arteries are blocked or the blockage is in a critical spot, a surgeon performs a bypass. They take a healthy blood vessel from your leg, arm, or chest and sew it around the blockage, creating a new route for blood to reach the heart muscle.
The New Frontier: Cardio-Oncology and Personalized Care
Medicine is moving toward a more personalized approach. We are seeing the rise of Cardio-oncology. Why? Because cancer treatments are getting better, people are surviving cancer longer, but some chemotherapy drugs can actually damage the heart or accelerate atherosclerosis. This requires a specialized team to manage both the cancer and the heart health simultaneously. Furthermore, the latest 2023 guidelines emphasize that we can't just treat the "blockage." We have to treat the person. This means adjusting the intensity of antithrombotic therapy based on whether a patient has other issues like atrial fibrillation or chronic kidney disease. The goal is to find the sweet spot where you prevent a heart attack without causing excessive bleeding.Can I reverse atherosclerosis?
While you cannot completely "erase" old plaques, you can stabilize them. Through aggressive LDL lowering (using statins) and lifestyle changes, plaques become denser and less likely to rupture, and in some cases, the volume of the plaque can slightly decrease. This significantly lowers the risk of a heart attack.
What is the difference between a heart attack and angina?
Angina is chest pain that happens because the heart muscle isn't getting enough oxygen-it's a warning sign. A heart attack (myocardial infarction) occurs when the blood flow is completely blocked, causing the heart muscle to actually start dying. Angina is a symptom; a heart attack is an acute event.
Do I need a stent if I have a 60% blockage?
Not necessarily. Many people with 60% blockages are managed perfectly well with medication and lifestyle changes, especially if they have no symptoms. Stents are typically reserved for cases where the blockage causes severe symptoms or when a blockage is causing an actual heart attack.
How does diabetes affect heart health?
High blood sugar levels over time damage the lining of the arteries (endothelial dysfunction), making it easier for cholesterol to build up. Diabetes also often comes with high blood pressure and weight gain, creating a "perfect storm" for the development of CAD.
Is a bypass surgery better than a stent?
It depends on the complexity. A stent (PCI) is less invasive and has a quicker recovery. However, for patients with "multi-vessel disease" (blockages in many different arteries) or those with diabetes, CABG (bypass) often provides better long-term outcomes and a lower risk of future heart attacks.






Been working in cardiology for years and the point about unstable plaques is so critical. People really think it's all about the percentage of the blockage, but a small rupture on a "thin cap" is what actually kills you. Just a heads up for anyone reading, if you're on blood thinners, keep a close eye on your bruising and always tell your dentist before any procedure!
Oh, the tragedy of the human condition! We spend our entire lives polishing the exterior of the vessel only for the internal plumbing to betray us in a sudden, violent crescendo of biological failure. It's practically a Shakespearean irony that the very organ pumping the essence of life is the one that chokes on its own greed for cholesterol. Truly, we are but fragile bags of salt and fat waiting for a plaque to decide our expiration date. How utterly bleak!
wow didnt know bout the calcium scan thing.. might be time to call doc :)
It can be incredibly overwhelming to receive a diagnosis like this, but I want everyone to know that there is so much hope and so many ways to turn things around if you just take it one small step at a time. Maybe start with a short walk today or swapping out one processed snack for a piece of fruit, because these tiny victories eventually add up to a much healthier heart and a longer life with the people you love, so please be gentle with yourselves during this journey.
The analogy of the engine is sufficient. Most people simply lack the discipline to maintain their biological machinery. It is quite simple: eat better and move more. The failure to do so is a choice, not a misfortune.
I totally get where Aubrey is coming from, but man, some of us just have the genetic lottery working against us. I've seen people eat salads and run marathons still end up with blockages because their bodies just love making LDL. It's kind of a bummer when you do everything "right" and your heart still decides to act up, but hey, that's just life, right?
Life is just a mirror of what we put into it. If you fill your body with junk, don't be shocked when your heart stops working. It's basic karma for your arteries.
The mention of endothelial dysfunction is pertinent. I wonder if the efficacy of SGLT2 inhibitors in mitigating cardiovascular events is specifically linked to the reduction of systemic inflammation or if it is primarily an osmotic effect on the renal system influencing preload and afterload.
I agree with the point about lifestyle changes. It's a good reminder for all of us to stay active and eat healthy. Thanks for sharing the info.
America has the best medical tech in the world for this! Our stents and bypass surgeries are way ahead of anywhere else. If you want the best care, you stay in the US!